
Yet another study is reported today that casts doubt on the value of supplementing vitamin D. Subjects were given either 400 iu daily or 50,000 iu twice a week. No difference in outcome was seen. I am going to agree with them for one minute here: I would not use either one of these options.
However, it boggles the mind that we are still so unsophisticated in our analyses of vitamin D. I present here a summary of studies that DID find a benefit. Since randomized studies of supplementation have not found harm, it seems the choice is whether to take a risk (that appears very small so far) to get an advantage as detailed below.
MAIN TAKEAWAY POINTS:
For this review, I have focused on randomized controlled trials of vitamin D supplementation.
Vitamin D supplementation in general, without regard to condition or level, generally reduces all-cause mortality (Chowdhury et al, 2014) and improves pregnancy outcomes (Sablok, 2015).
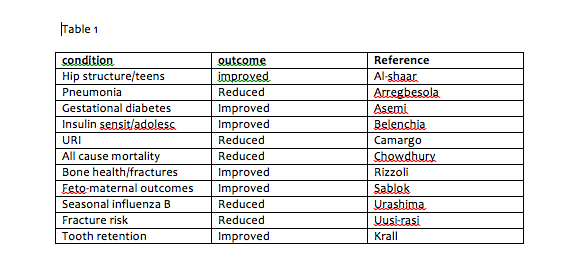
The most obvious benefit of vitamin D supplementation is for people whose vitamin D is below 20 ng/mL. In my opinion, this group makes it worthwhile to screen everyone with a vitamin D level, as supplemented patients will experience fewer bone fractures, less injury from falls, better tooth retention, better sleep and well being, less overall pain, less cardiovascular disease, less asthma and COPD, less influenza, fewer colds, and less pneumonia (see Table 1).
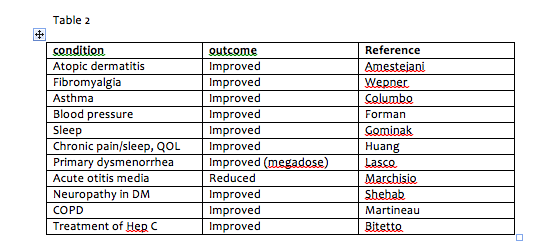
If people already have certain medical conditions, raising vitamin D using supplements will help them to have better outcomes with Hepatitis C treatment, to have less joint pain (with rheumatoid arthritis), less neuropathy (with diabetes), less pain (with fibromyalgia), better glucose control (with gestational diabetes), lowered insulin resistance (teenagers with prediabetes), less eczema, and fewer episodes of otitis media (for children prone to otitis) (see Table 2).
However, it boggles the mind that we are still so unsophisticated in our analyses of vitamin D. I present here a summary of studies that DID find a benefit. Since randomized studies of supplementation have not found harm, it seems the choice is whether to take a risk (that appears very small so far) to get an advantage as detailed below.
MAIN TAKEAWAY POINTS:
- Vitamin D supplementation is beneficial in a number of conditions and especially for patients below the 20 ng/mL cutoff
- The dose of vitamin D is about 100 iu daily of vitamin D3 for each 1 ng/mL you want to increase the level by, double that for obese patient
- Toxicity is unusual, but possible with doses above 10,000 iu daily
- The ideal level to aim for may depend on the condition and the patient’s genetics; 50 ng/mL is reasonable, but levels up to 60-80 ng/mL or even 80-90 ng/mL have their supporters
For this review, I have focused on randomized controlled trials of vitamin D supplementation.
Vitamin D supplementation in general, without regard to condition or level, generally reduces all-cause mortality (Chowdhury et al, 2014) and improves pregnancy outcomes (Sablok, 2015).
The most obvious benefit of vitamin D supplementation is for people whose vitamin D is below 20 ng/mL. In my opinion, this group makes it worthwhile to screen everyone with a vitamin D level, as supplemented patients will experience fewer bone fractures, less injury from falls, better tooth retention, better sleep and well being, less overall pain, less cardiovascular disease, less asthma and COPD, less influenza, fewer colds, and less pneumonia (see Table 1).
If people already have certain medical conditions, raising vitamin D using supplements will help them to have better outcomes with Hepatitis C treatment, to have less joint pain (with rheumatoid arthritis), less neuropathy (with diabetes), less pain (with fibromyalgia), better glucose control (with gestational diabetes), lowered insulin resistance (teenagers with prediabetes), less eczema, and fewer episodes of otitis media (for children prone to otitis) (see Table 2).
One study compared gene expression in people with low vs. normal vitamin D levels. They found 66 genes expressing differently between the two groups. In vitamin D deficient subject, supplementation corrected the expression of these genes (Hossein-nezhad et al, 2014).
The expression of several immunological markers was improved in a group of patients with multiple sclerosis supplemented to a average level of 50 ng/mL (Terrier et al, 2012).
In many cases, research has not shown a benefit to attaining levels above 35 ng/mL, and there are concerns that there may be adverse consequences of excessive vitamin D supplementation. However, it is hard to draw firm conclusions in that regard. Few research subjects attain levels much above 35 ng/mL, making it difficult to find statistically significant differences above that level. The studies showing associations between high vitamin D levels and certain illnesses do not involve a randomized controlled comparison of people taking different doses of vitamin D. This introduces the possibility that there are other reasons people with high vitamin D levels sometimes have higher fracture risk (Bleicher et al, 2014), more Type 1 diabetes (Gorham et al, 2012) or higher risk of cardiovascular disease.
For certain conditions, a vitamin D level above 40 ng/mL is the most beneficial (Munger et al, 2006). In fibromyalgia, maximum benefit was found when patients were supplemented to levels exceeding 48 ng/mL (Wepner et al, 2014). Some neurologists (Gominak et al, 2012) claim that it is necessary to supplement patients to levels of 60-80 ng/mL to correct sleep problems, including sleep apnea, and levels above 80 ng/mL may offer additional advantages in autism (Cannell, personal communication; Perlmutter—in his book, Grain Brain).
Some people have genetics that result in lower vitamin D levels (Wang et al, 2011). These variants are near genes involved in cholesterol synthesis, hydroxylation and vitamin D transport. There are also inborn errors of vitamin D metabolism, some of which can be overcome with vitamin D supplementation (Malloy et al, 2010).
Some people also have genetics that impair the hydroxylation of 25 OH vitamin D to the active form 1, 25 OH vitamin D. It is tempting to hypothesize that these are the patients who get more benefit from very high levels. Mitochondria are involved in this conversion, raising the possibility that mitochondrial dysfunction also impacts need for high levels of 25 OH vitamin D (See Perfect Health Diet website).
Vitamin D supplementation as a single 300,000 iu dose can also be used to treat primary dysmenorrhea (Lasco et al, 2012).
I would love to find research support for an ideal level being in the 50ng/mL, or the 70-80+ range. This is frequently recommended in functional medicine, but does not appear well supported, and certainly not by randomized controlled studies of supplementation.
Please comment if you have studies to support aiming for such a high level!
REFERENCES
Al-Shaar L1, Nabulsi M, Maalouf J, El-Rassi R, Vieth R, Beck TJ, El-Hajj Fuleihan G.
Bone. 2013 Oct;56(2):296-303. Effect of vitamin D replacement on hip structural geometry in adolescents: a randomized controlled trial.
Amestejani M, Salehi BS, Vasigh M, Sobhkhiz A, Karami M, Alinia H, Kamrava SK, Shamspour N, Ghalehbaghi B, Behzadi AH. J Drugs Dermatol. 2012 Mar;11(3):327-30.
Vitamin D supplementation in the treatment of atopic dermatitis: a clinical trial study.
Arregbesola et al. J Epidemiol Community Health Serum 25-hydroxyvitamin D3 and the risk of pneumonia in an ageing general population. (huge connection with deficiency; when sufficient, no added benefit).
Asemi Z & Maryam Karamali &Ahmad Esmaillzadeh .Diabetologia 2014 Effects of calcium–vitamin D co-supplementation on glycaemic control, inflammation and oxidative stress in gestational diabetes:a randomised placebo-controlled trial
Belenchia AM, Tosh AK, Hillman LS, Peterson CA.; Am J Clin Nutr. 2013 Apr;97(4):774-81. Correcting vitamin D insufficiency improves insulin sensitivity in obese adolescents: a randomized controlled trial.
Bleicher K1, Cumming RG, Naganathan V, Blyth FM, Le Couteur DG, Handelsman DJ, Waite LM, Seibel MJ. J Bone Miner Res. 2014 Sep;29(9):2024-31.
U-shaped association between serum 25-hydroxyvitamin D and fracture risk in older men: results from the prospective population-based CHAMP study.
Bitetto D1, Fabris C, Fornasiere E, Pipan C, Fumolo E, Cussigh A, Bignulin S, Cmet S, Fontanini E, Falleti E, Martinella R, Pirisi M, Toniutto P. Transpl Int. 2011 Jan;24(1):43-50. Vitamin D supplementation improves response to antiviral treatment for recurrent hepatitis C.
Camargo CA Jr, Ganmaa D, Frazier AL, Kirchberg FF, Stuart JJ, Kleinman K, Sumberzul N, Rich-Edwards JW. Pediatrics. 2012 Sep;130(3):e561-7. Randomized trial of vitamin D supplementation and risk of acute respiratory infection in Mongolia.
Chowdhury Rajiv, Kunutsor Setor, Vitezova Anna, Oliver Williams Clare, Chowdhury Susmita, Kiefte-de-Jong Jessica C et al. Vitamin D and risk of cause specific death: systematic review and meta-analysis of observational cohort and randomised intervention studies BMJ 2014
Columbo M, Reynold A Panettieri2 and Albert S Rohr1Allergy, Ashtma and Clinical Immunology 2014 Asthma in the elderly: a study of the role of vitamin D;
Forman JP1, Scott JB, Ng K, Drake BF, Suarez EG, Hayden DL, Bennett GG, Chandler PD, Hollis BW, Emmons KM, Giovannucci EL, Fuchs CS, Chan AT
Hypertension. 2013 Apr;61(4):779-85.
Effect of vitamin D supplementation on blood pressure in blacks.
Gominak SC1, Stumpf WE.
Med Hypotheses. 2012 Aug;79(2):132-5. doi: 10.1016/j.mehy.2012.03.031. Epub 2012 May 13. The world epidemic of sleep disorders is linked to vitamin D deficiency.
Gorham, ED & C. F. Garland & A. A. Burgi & S. B. Mohr & K. Zeng & H. Hofflich & J. J. Kim & C. Ricordi. Diabetologia 2012 Lower prediagnostic serum 25-hydroxyvitamin D concentration is associated with higher risk of insulin-requiring diabetes: a nested case–control study (another U shaped curve, T1DM)
Greene DA1, Naughton GA. Osteoporos Int. 2011 Feb;22(2):489-98. Calcium and vitamin-D supplementation on bone structural properties in peripubertal female identical twins: a randomised controlled trial.
Hossein-nezhad A, Spira A, Holick MF. PLoS One. 2013;8(3):e58725. Influence of vitamin D status and vitamin D3 supplementation on genome wide expression of white blood cells: a randomized double-blind clinical trial.
Hong Q, Xu J, Xu S, Lian L, Zhang M, Ding C. Rheumatology (Oxford). 2014 Nov;53(11):1994-2001. Associations between serum 25-hydroxyvitamin D and disease activity, inflammatory cytokines and bone loss in patients with rheumatoid arthritis.
Huang W1, Shah S, Long Q, Crankshaw AK, Tangpricha V. Clin J Pain. 2013 Apr;29(4):341-7. Improvement of pain, sleep, and quality of life in chronic pain patients with vitamin D supplementation.
Krall EA, Wehler C, Garcia RI, Harris SS, Dawson-Hughes B.Am J Med. 2001 Oct 15;111(6):452-6. Calcium and vitamin D supplements reduce tooth loss in the elderly.
Lasco A, Catalano A, Benvenga S. Improvement of Primary Dysmenorrhea Caused by a Single Oral Dose of Vitamin D: Results of a Randomized, Double-blind, Placebo-Controlled Study. Arch Intern Med.2012;172(4):366-367.
Malloy PJ, Feldman D. Genetic Disorders and Defects in Vitamin D Action.Endocrinology and metabolism clinics of North America. 2010;39(2):333-346
Marchisio P1, Consonni D, Baggi E, Zampiero A, Bianchini S, Terranova L, Tirelli S, Esposito S, Principi N.Pediatr Infect Dis J. 2013 Oct;32(10):1055-60.
Vitamin D supplementation reduces the risk of acute otitis media in otitis-prone children. (took kids over 30ng/dl, using 1000 iu vitamin D, to prevent ear infections)
Martineau AR et al. Lancet Respiratory Medicine 2014. Vitamin D3 supplementation in patients with chronic obstructive pulmonary disease (ViDiCO): a multicentre, double-blind, randomised controlled trial (only people who start out deficient improve, about 2000 iu daily is enough; they attain about 35 ng at most by the time they are done)
Munger KL, Levin LI, Hollis BW, Howard NS, Ascherio A.
JAMA. 2006 Dec 20;296(23):2832-8.
Serum 25-hydroxyvitamin D levels and risk of multiple sclerosis.
Shehab D.a · Al-Jarallah K.a · Abdella N.a · Mojiminiyi O.A.b · Al Mohamedy H. Medical Principles and Practice 2015 Prospective Evaluation of the Effect of Short-Term Oral Vitamin D Supplementation on Peripheral Neuropathy in Type 2 Diabetes
Rizzoli R, Boonen S, Brandi ML, Bruyère O, Cooper C, Kanis JA, Kaufman JM, Ringe JD, Weryha G, Reginster JY. Curr Med Res Opin. 2013 Apr;29(4):305-13.
Vitamin D supplementation in elderly or postmenopausal women: a 2013 update of the 2008 recommendations from the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO).
Sablok A1, Batra A, Thariani K, Batra A, Bharti R, Aggarwal AR, Kabi BC, Chellani H.
Clin Endocrinol (Oxf). 2015 Feb 14. Supplementation of vitamin D in pregnancy and its correlation with feto-maternal outcome.
Terrier B, Derian N, Schoindre Y, Chaara W, Geri G, Zahr N, Mariampillai K, Rosenzwajg M, Carpentier W, Musset L, Piette JC, Six A, Klatzmann D, Saadoun D,Patrice C, Costedoat-Chalumeau N. Arthritis Res Ther. 2012 Oct 17;14(5):R221.
Restoration of regulatory and effector T cell balance and B cell homeostasis in systemic lupus erythematosus patients through vitamin D supplementation.
Urashima M, Segawa T, Okazaki M, Kurihara M, Wada Y, Ida H.
Am J Clin Nutr. 2010 May;91(5):1255-60. Randomized trial of vitamin D supplementation to prevent seasonal influenza A in schoolchildren.
Uusi-Rasi K, Patil R, Karinkanta S, et al. Exercise and Vitamin D in Fall Prevention Among Older Women: A Randomized Clinical Trial. JAMA Intern Med. Published online March 23, 2015.
Wang et al (very large group). Lancet. 2010 Jul 17;376(9736):180-8.
Common genetic determinants of vitamin D insufficiency: a genome-wide association study.
Wepner F, Raphael Scheuer, Birgit Schuetz-Wieser, Peter Machacek, Elisabeth Pieler-Bruha, Heide S. Cross, Julia Hahne, Martin Friedrich Pain 2014 Effects of vitamin D on patients with fibromyalgia syndrome: A randomized placebo-controlled trial (this group attained a level of 48 ng or more; pain resumed 6m after supplementation stopped)
Wepner F, Raphael Scheuer, Birgit Schuetz-Wieser, Peter Machacek, Elisabeth Pieler-Bruha, Heide S. Cross, Julia Hahne, Martin Friedrich
Arthritis Research and Therapy 2012. Effects of vitamin D on patients with fibromyalgia syndrome: A randomized placebo-controlled trial.
The expression of several immunological markers was improved in a group of patients with multiple sclerosis supplemented to a average level of 50 ng/mL (Terrier et al, 2012).
In many cases, research has not shown a benefit to attaining levels above 35 ng/mL, and there are concerns that there may be adverse consequences of excessive vitamin D supplementation. However, it is hard to draw firm conclusions in that regard. Few research subjects attain levels much above 35 ng/mL, making it difficult to find statistically significant differences above that level. The studies showing associations between high vitamin D levels and certain illnesses do not involve a randomized controlled comparison of people taking different doses of vitamin D. This introduces the possibility that there are other reasons people with high vitamin D levels sometimes have higher fracture risk (Bleicher et al, 2014), more Type 1 diabetes (Gorham et al, 2012) or higher risk of cardiovascular disease.
For certain conditions, a vitamin D level above 40 ng/mL is the most beneficial (Munger et al, 2006). In fibromyalgia, maximum benefit was found when patients were supplemented to levels exceeding 48 ng/mL (Wepner et al, 2014). Some neurologists (Gominak et al, 2012) claim that it is necessary to supplement patients to levels of 60-80 ng/mL to correct sleep problems, including sleep apnea, and levels above 80 ng/mL may offer additional advantages in autism (Cannell, personal communication; Perlmutter—in his book, Grain Brain).
Some people have genetics that result in lower vitamin D levels (Wang et al, 2011). These variants are near genes involved in cholesterol synthesis, hydroxylation and vitamin D transport. There are also inborn errors of vitamin D metabolism, some of which can be overcome with vitamin D supplementation (Malloy et al, 2010).
Some people also have genetics that impair the hydroxylation of 25 OH vitamin D to the active form 1, 25 OH vitamin D. It is tempting to hypothesize that these are the patients who get more benefit from very high levels. Mitochondria are involved in this conversion, raising the possibility that mitochondrial dysfunction also impacts need for high levels of 25 OH vitamin D (See Perfect Health Diet website).
Vitamin D supplementation as a single 300,000 iu dose can also be used to treat primary dysmenorrhea (Lasco et al, 2012).
I would love to find research support for an ideal level being in the 50ng/mL, or the 70-80+ range. This is frequently recommended in functional medicine, but does not appear well supported, and certainly not by randomized controlled studies of supplementation.
Please comment if you have studies to support aiming for such a high level!
REFERENCES
Al-Shaar L1, Nabulsi M, Maalouf J, El-Rassi R, Vieth R, Beck TJ, El-Hajj Fuleihan G.
Bone. 2013 Oct;56(2):296-303. Effect of vitamin D replacement on hip structural geometry in adolescents: a randomized controlled trial.
Amestejani M, Salehi BS, Vasigh M, Sobhkhiz A, Karami M, Alinia H, Kamrava SK, Shamspour N, Ghalehbaghi B, Behzadi AH. J Drugs Dermatol. 2012 Mar;11(3):327-30.
Vitamin D supplementation in the treatment of atopic dermatitis: a clinical trial study.
Arregbesola et al. J Epidemiol Community Health Serum 25-hydroxyvitamin D3 and the risk of pneumonia in an ageing general population. (huge connection with deficiency; when sufficient, no added benefit).
Asemi Z & Maryam Karamali &Ahmad Esmaillzadeh .Diabetologia 2014 Effects of calcium–vitamin D co-supplementation on glycaemic control, inflammation and oxidative stress in gestational diabetes:a randomised placebo-controlled trial
Belenchia AM, Tosh AK, Hillman LS, Peterson CA.; Am J Clin Nutr. 2013 Apr;97(4):774-81. Correcting vitamin D insufficiency improves insulin sensitivity in obese adolescents: a randomized controlled trial.
Bleicher K1, Cumming RG, Naganathan V, Blyth FM, Le Couteur DG, Handelsman DJ, Waite LM, Seibel MJ. J Bone Miner Res. 2014 Sep;29(9):2024-31.
U-shaped association between serum 25-hydroxyvitamin D and fracture risk in older men: results from the prospective population-based CHAMP study.
Bitetto D1, Fabris C, Fornasiere E, Pipan C, Fumolo E, Cussigh A, Bignulin S, Cmet S, Fontanini E, Falleti E, Martinella R, Pirisi M, Toniutto P. Transpl Int. 2011 Jan;24(1):43-50. Vitamin D supplementation improves response to antiviral treatment for recurrent hepatitis C.
Camargo CA Jr, Ganmaa D, Frazier AL, Kirchberg FF, Stuart JJ, Kleinman K, Sumberzul N, Rich-Edwards JW. Pediatrics. 2012 Sep;130(3):e561-7. Randomized trial of vitamin D supplementation and risk of acute respiratory infection in Mongolia.
Chowdhury Rajiv, Kunutsor Setor, Vitezova Anna, Oliver Williams Clare, Chowdhury Susmita, Kiefte-de-Jong Jessica C et al. Vitamin D and risk of cause specific death: systematic review and meta-analysis of observational cohort and randomised intervention studies BMJ 2014
Columbo M, Reynold A Panettieri2 and Albert S Rohr1Allergy, Ashtma and Clinical Immunology 2014 Asthma in the elderly: a study of the role of vitamin D;
Forman JP1, Scott JB, Ng K, Drake BF, Suarez EG, Hayden DL, Bennett GG, Chandler PD, Hollis BW, Emmons KM, Giovannucci EL, Fuchs CS, Chan AT
Hypertension. 2013 Apr;61(4):779-85.
Effect of vitamin D supplementation on blood pressure in blacks.
Gominak SC1, Stumpf WE.
Med Hypotheses. 2012 Aug;79(2):132-5. doi: 10.1016/j.mehy.2012.03.031. Epub 2012 May 13. The world epidemic of sleep disorders is linked to vitamin D deficiency.
Gorham, ED & C. F. Garland & A. A. Burgi & S. B. Mohr & K. Zeng & H. Hofflich & J. J. Kim & C. Ricordi. Diabetologia 2012 Lower prediagnostic serum 25-hydroxyvitamin D concentration is associated with higher risk of insulin-requiring diabetes: a nested case–control study (another U shaped curve, T1DM)
Greene DA1, Naughton GA. Osteoporos Int. 2011 Feb;22(2):489-98. Calcium and vitamin-D supplementation on bone structural properties in peripubertal female identical twins: a randomised controlled trial.
Hossein-nezhad A, Spira A, Holick MF. PLoS One. 2013;8(3):e58725. Influence of vitamin D status and vitamin D3 supplementation on genome wide expression of white blood cells: a randomized double-blind clinical trial.
Hong Q, Xu J, Xu S, Lian L, Zhang M, Ding C. Rheumatology (Oxford). 2014 Nov;53(11):1994-2001. Associations between serum 25-hydroxyvitamin D and disease activity, inflammatory cytokines and bone loss in patients with rheumatoid arthritis.
Huang W1, Shah S, Long Q, Crankshaw AK, Tangpricha V. Clin J Pain. 2013 Apr;29(4):341-7. Improvement of pain, sleep, and quality of life in chronic pain patients with vitamin D supplementation.
Krall EA, Wehler C, Garcia RI, Harris SS, Dawson-Hughes B.Am J Med. 2001 Oct 15;111(6):452-6. Calcium and vitamin D supplements reduce tooth loss in the elderly.
Lasco A, Catalano A, Benvenga S. Improvement of Primary Dysmenorrhea Caused by a Single Oral Dose of Vitamin D: Results of a Randomized, Double-blind, Placebo-Controlled Study. Arch Intern Med.2012;172(4):366-367.
Malloy PJ, Feldman D. Genetic Disorders and Defects in Vitamin D Action.Endocrinology and metabolism clinics of North America. 2010;39(2):333-346
Marchisio P1, Consonni D, Baggi E, Zampiero A, Bianchini S, Terranova L, Tirelli S, Esposito S, Principi N.Pediatr Infect Dis J. 2013 Oct;32(10):1055-60.
Vitamin D supplementation reduces the risk of acute otitis media in otitis-prone children. (took kids over 30ng/dl, using 1000 iu vitamin D, to prevent ear infections)
Martineau AR et al. Lancet Respiratory Medicine 2014. Vitamin D3 supplementation in patients with chronic obstructive pulmonary disease (ViDiCO): a multicentre, double-blind, randomised controlled trial (only people who start out deficient improve, about 2000 iu daily is enough; they attain about 35 ng at most by the time they are done)
Munger KL, Levin LI, Hollis BW, Howard NS, Ascherio A.
JAMA. 2006 Dec 20;296(23):2832-8.
Serum 25-hydroxyvitamin D levels and risk of multiple sclerosis.
Shehab D.a · Al-Jarallah K.a · Abdella N.a · Mojiminiyi O.A.b · Al Mohamedy H. Medical Principles and Practice 2015 Prospective Evaluation of the Effect of Short-Term Oral Vitamin D Supplementation on Peripheral Neuropathy in Type 2 Diabetes
Rizzoli R, Boonen S, Brandi ML, Bruyère O, Cooper C, Kanis JA, Kaufman JM, Ringe JD, Weryha G, Reginster JY. Curr Med Res Opin. 2013 Apr;29(4):305-13.
Vitamin D supplementation in elderly or postmenopausal women: a 2013 update of the 2008 recommendations from the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO).
Sablok A1, Batra A, Thariani K, Batra A, Bharti R, Aggarwal AR, Kabi BC, Chellani H.
Clin Endocrinol (Oxf). 2015 Feb 14. Supplementation of vitamin D in pregnancy and its correlation with feto-maternal outcome.
Terrier B, Derian N, Schoindre Y, Chaara W, Geri G, Zahr N, Mariampillai K, Rosenzwajg M, Carpentier W, Musset L, Piette JC, Six A, Klatzmann D, Saadoun D,Patrice C, Costedoat-Chalumeau N. Arthritis Res Ther. 2012 Oct 17;14(5):R221.
Restoration of regulatory and effector T cell balance and B cell homeostasis in systemic lupus erythematosus patients through vitamin D supplementation.
Urashima M, Segawa T, Okazaki M, Kurihara M, Wada Y, Ida H.
Am J Clin Nutr. 2010 May;91(5):1255-60. Randomized trial of vitamin D supplementation to prevent seasonal influenza A in schoolchildren.
Uusi-Rasi K, Patil R, Karinkanta S, et al. Exercise and Vitamin D in Fall Prevention Among Older Women: A Randomized Clinical Trial. JAMA Intern Med. Published online March 23, 2015.
Wang et al (very large group). Lancet. 2010 Jul 17;376(9736):180-8.
Common genetic determinants of vitamin D insufficiency: a genome-wide association study.
Wepner F, Raphael Scheuer, Birgit Schuetz-Wieser, Peter Machacek, Elisabeth Pieler-Bruha, Heide S. Cross, Julia Hahne, Martin Friedrich Pain 2014 Effects of vitamin D on patients with fibromyalgia syndrome: A randomized placebo-controlled trial (this group attained a level of 48 ng or more; pain resumed 6m after supplementation stopped)
Wepner F, Raphael Scheuer, Birgit Schuetz-Wieser, Peter Machacek, Elisabeth Pieler-Bruha, Heide S. Cross, Julia Hahne, Martin Friedrich
Arthritis Research and Therapy 2012. Effects of vitamin D on patients with fibromyalgia syndrome: A randomized placebo-controlled trial.







 RSS Feed
RSS Feed
